Anatomical considerations Corneal
![]()
![]()
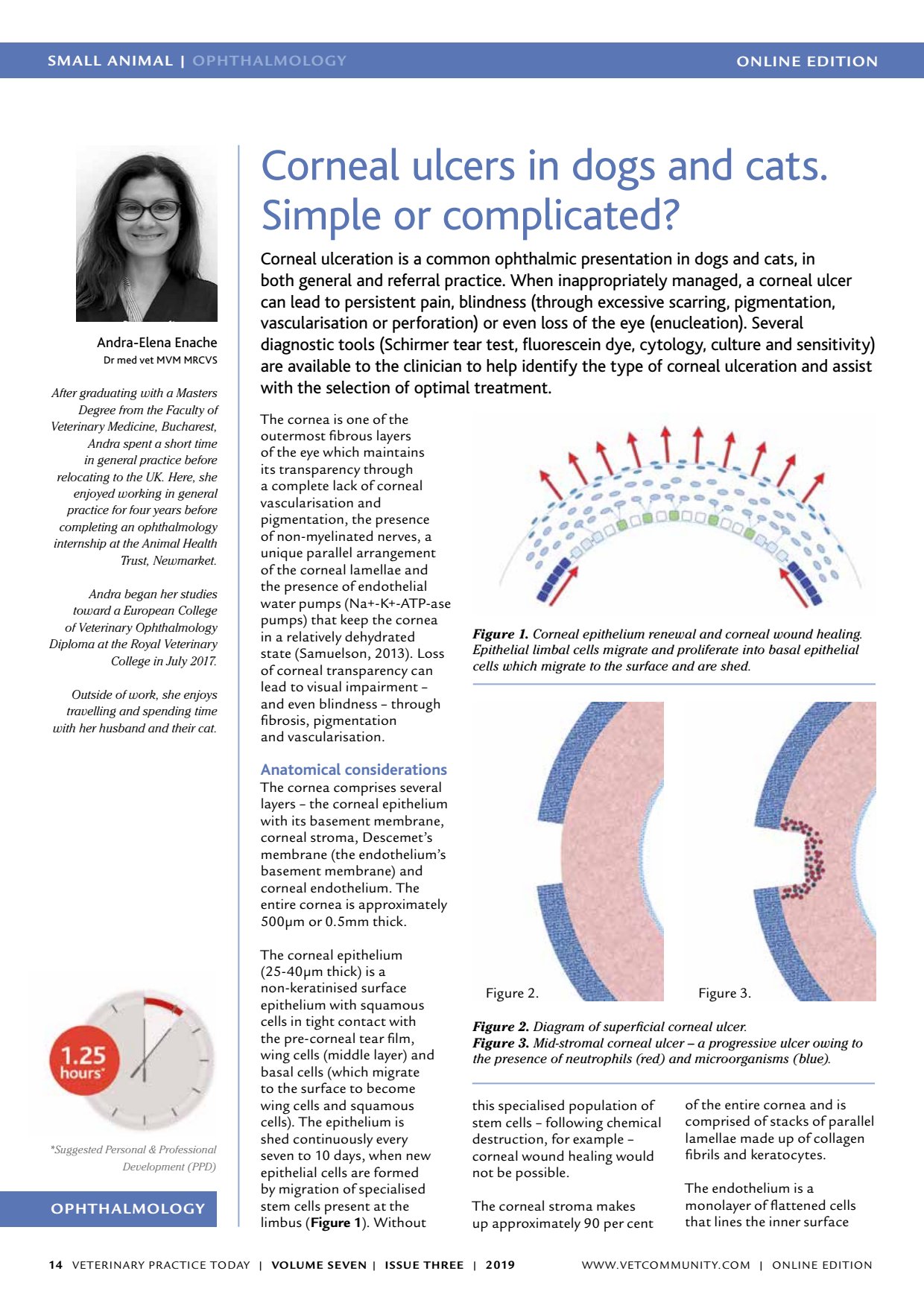
ONLINE EDITIONSMALL ANIMAL | OPHTHALMOLOGY VETERINARY PRACTICE TODAY | VOLUME SEVEN | ISSUE THREE | 2019 14 OPHTHALMOLOGY Suggested Personal & Professional Development (PPD) Andra-Elena Enache Dr med vet MVM MRCVS After graduating with a Masters Degree from the Faculty of Veterinary Medicine, Bucharest, Andra spent a short time in general practice before relocating to the UK. Here, she enjoyed working in general practice for four years before completing an ophthalmology internship at the Animal Health Trust, Newmarket. Andra began her studies toward a European College of Veterinary Ophthalmology Diploma at the Royal Veterinary College in July 2017. Outside of work, she enjoys travelling and spending time with her husband and their cat. Corneal ulcers in dogs and cats. Simple or complicated? Corneal ulceration is a common ophthalmic presentation in dogs and cats, in both general and referral practice. When inappropriately managed, a corneal ulcer can lead to persistent pain, blindness (through excessive scarring, pigmentation, vascularisation or perforation) or even loss of the eye (enucleation). Several diagnostic tools (Schirmer tear test, fluorescein dye, cytology, culture and sensitivity) are available to the clinician to help identify the type of corneal ulceration and assist with the selection of optimal treatment. The cornea is one of the outermost fibrous layers of the eye which maintains its transparency through a complete lack of corneal vascularisation and pigmentation, the presence of non-myelinated nerves, a unique parallel arrangement of the corneal lamellae and the presence of endothelial water pumps (Na+-K+-ATP-ase pumps) that keep the cornea in a relatively dehydrated state (Samuelson, 2013). Loss of corneal transparency can lead to visual impairment and even blindness through fibrosis, pigmentation and vascularisation. Anatomical considerations The cornea comprises several layers the corneal epithelium with its basement membrane, corneal stroma, Descemets membrane (the endotheliums basement membrane) and corneal endothelium. The entire cornea is approximately 500µm or 0.5mm thick. The corneal epithelium (25-40µm thick) is a non-keratinised surface epithelium with squamous cells in tight contact with the pre-corneal tear film, wing cells (middle layer) and basal cells (which migrate to the surface to become wing cells and squamous cells). The epithelium is shed continuously every seven to 10 days, when new epithelial cells are formed by migration of specialised stem cells present at the limbus ( Figure 1 ). Without this specialised population of stem cells following chemical destruction, for example corneal wound healing would not be possible. The corneal stroma makes up approximately 90 per cent of the entire cornea and is comprised of stacks of parallel lamellae made up of collagen fibrils and keratocytes. The endothelium is a monolayer of flattened cells that lines the inner surface Figure 1. Corneal epithelium renewal and corneal wound healing. Epithelial limbal cells migrate and proliferate into basal epithelial cells which migrate to the surface and are shed. Figure 2. Diagram of superficial corneal ulcer. Figure 3. Mid-stromal corneal ulcer a progressive ulcer owing to the presence of neutrophils (red) and microorganisms (blue). Figure 3. Figure 2. WWW.VETCOMMUNIT Y.COM | ONLINE EDITION