Bacterial pathogenicity invasiveness
![]()
![]()
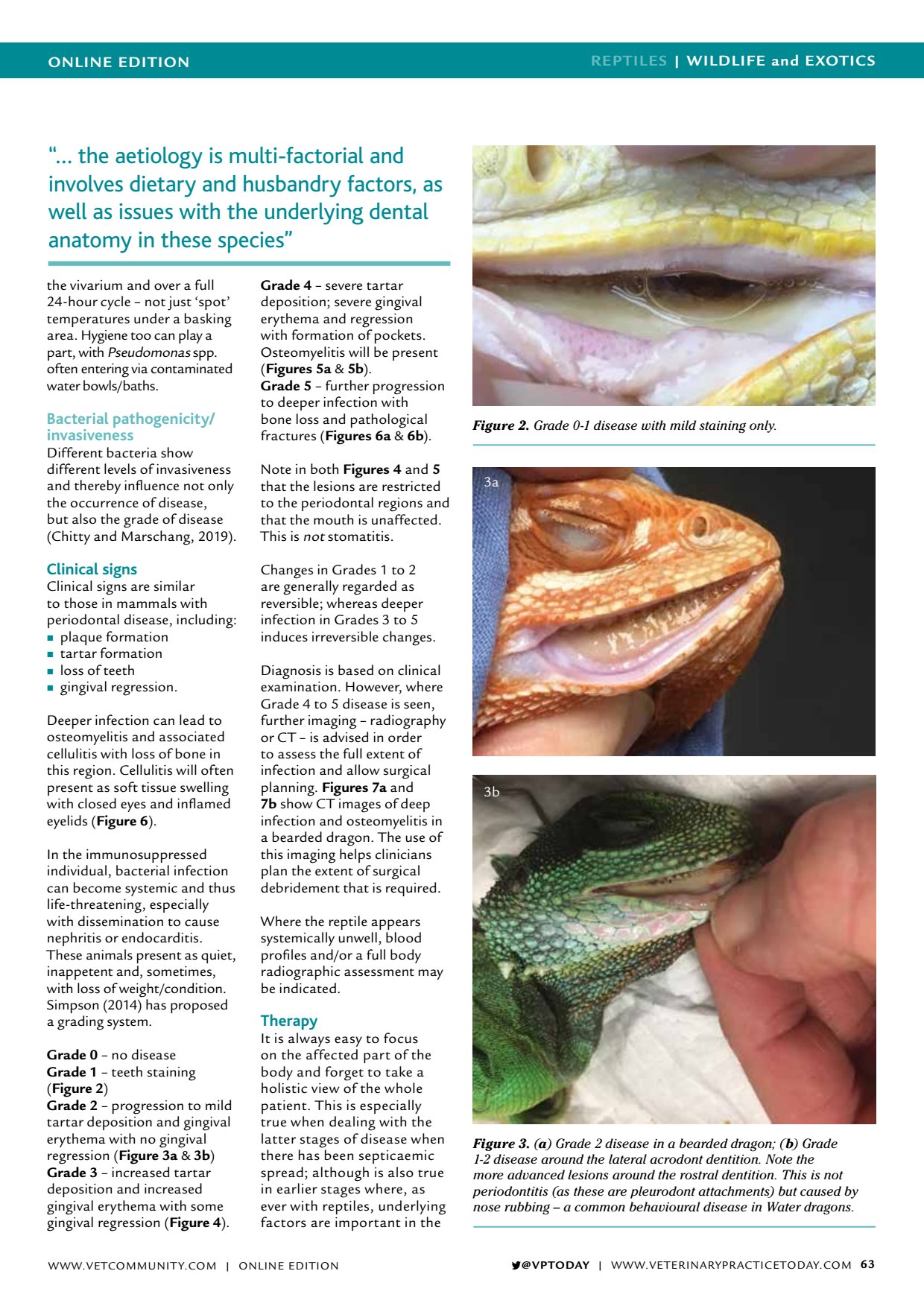
ONLINE EDITION REPTILES | WILDLIFE and EXOTICS VPTODAY | WWW.VETERINARYPRACTICETODAY.COM 63 the vivarium and over a full 24-hour cycle not just spot temperatures under a basking area. Hygiene too can play a part, with Pseudomonas spp. often entering via contaminated water bowls/baths. Bacterial pathogenicity/ invasiveness Different bacteria show different levels of invasiveness and thereby influence not only the occurrence of disease, but also the grade of disease (Chitty and Marschang, 2019). Clinical signs Clinical signs are similar to those in mammals with periodontal disease, including: plaque formation tartar formation loss of teeth gingival regression. Deeper infection can lead to osteomyelitis and associated cellulitis with loss of bone in this region. Cellulitis will often present as soft tissue swelling with closed eyes and inflamed eyelids ( Figure 6 ). In the immunosuppressed individual, bacterial infection can become systemic and thus life-threatening, especially with dissemination to cause nephritis or endocarditis. These animals present as quiet, inappetent and, sometimes, with loss of weight/condition. Simpson (2014) has proposed a grading system. Grade 0 no disease Grade 1 teeth staining ( Figure 2 ) Grade 2 progression to mild tartar deposition and gingival erythema with no gingival regression ( Figure 3a & 3b ) Grade 3 increased tartar deposition and increased gingival erythema with some gingival regression ( Figure 4 ). Grade 4 severe tartar deposition; severe gingival erythema and regression with formation of pockets. Osteomyelitis will be present ( Figures 5a & 5b ). Grade 5 further progression to deeper infection with bone loss and pathological fractures ( Figures 6a & 6b ). Note in both Figures 4 and 5 that the lesions are restricted to the periodontal regions and that the mouth is unaffected. This is not stomatitis. Changes in Grades 1 to 2 are generally regarded as reversible; whereas deeper infection in Grades 3 to 5 induces irreversible changes. Diagnosis is based on clinical examination. However, where Grade 4 to 5 disease is seen, further imaging radiography or CT is advised in order to assess the full extent of infection and allow surgical planning. Figures 7a and 7b show CT images of deep infection and osteomyelitis in a bearded dragon. The use of this imaging helps clinicians plan the extent of surgical debridement that is required. Where the reptile appears systemically unwell, blood profiles and/or a full body radiographic assessment may be indicated. Therapy It is always easy to focus on the affected part of the body and forget to take a holistic view of the whole patient. This is especially true when dealing with the latter stages of disease when there has been septicaemic spread; although is also true in earlier stages where, as ever with reptiles, underlying factors are important in the Figure 2. Grade 0-1 disease with mild staining only. Figure 3. ( a ) Grade 2 disease in a bearded dragon; ( b ) Grade 1-2 disease around the lateral acrodont dentition. Note the more advanced lesions around the rostral dentition. This is not periodontitis (as these are pleurodont attachments) but caused by nose rubbing a common behavioural disease in Water dragons. 3a 3b the aetiology is multi-factorial and involves dietary and husbandry factors, as well as issues with the underlying dental anatomy in these species WWW.VETCOMMUNIT Y.COM | ONLINE EDITION